
The Five Common Prescriptions That Destroy a Man’s Health
And why aren't doctors telling men this?

Every year, American doctors write over four billion prescriptions.
Four billion.
That is not a typo. The average American adult now takes four prescription medications. If you’re over sixty-five, it’s closer to seven.
We have become the most medicated society in the history of the human race.
And nobody is asking the obvious question: What are all these drugs doing to us?
Not what are they doing to the symptom they’re prescribed for. That part is usually fine. Your cholesterol number goes down. Your blood pressure number goes down. Your acid reflux goes away. The lab report looks better.
But what is happening to the man taking the pill?
The answer, backed by study after study, is disturbing. Somehow doctors hardly ever tell patients any of this stuff.
So, The Cookster (that’s me) -- is going to walk you through five of the most commonly prescribed medications in America.
Drugs your doctor has probably prescribed to you or someone you know. Drugs that are considered safe, standard, routine.
And I’m going to show you what the research says they’re quietly doing to your testosterone, your energy, your sexual function, your brain, and your body — while your doctor tells you everything is fine.
Quick disclaimer: I’m not your doctor. I’m not a doctor. If you get some ideas from this, ask your doctor about it. Don’t ever adjust your medications without asking your doctor first. End of disclaimer. Let’s move on to the meat.
1. Statins — The Cholesterol Drug That Lowers More Than Cholesterol
Statins are the most prescribed class of drug in America. Over 40 million Americans take one. Lipitor, Crestor, Zocor — you know the names. Your doctor probably pushed one on you the moment your total cholesterol crept above 200.
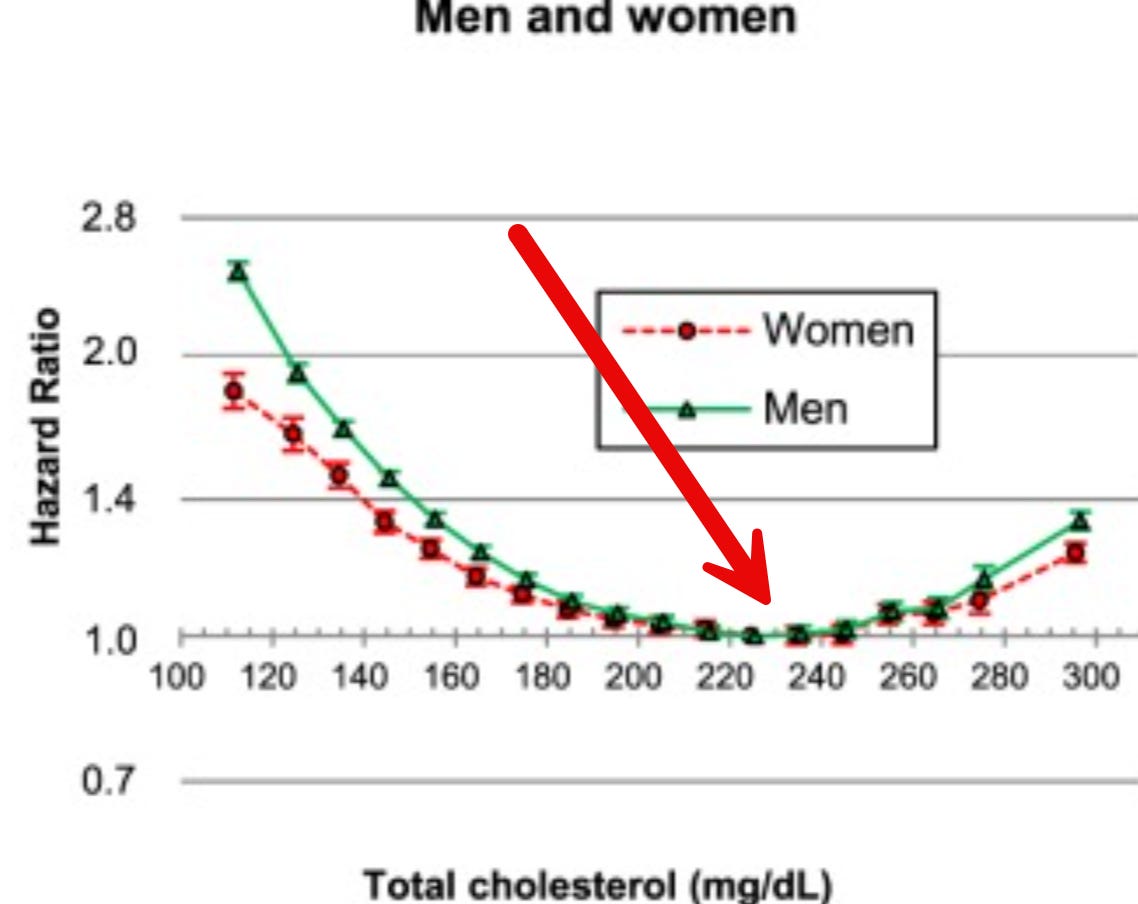
There’s lots of arguments against cholesterol. I’ve often shown men that the ideal cholesterol level is around 220 to 240. That’s where the all-cause mortality is the lowest.
See the red arrow...This is a study with seventeen million people. It’s a long-term study, and there are many such studies.
No valid, decently run studies ever shown that lowering cholesterol below 220-240 is actually increasing your longevity.
Here’s what else your doctor didn’t tell you.
Statins work by inhibiting an enzyme called HMG-CoA reductase. That enzyme is part of the pathway your body uses to make cholesterol. But that same pathway — the mevalonate pathway — is also how your body makes CoQ10, a molecule that is absolutely essential for cellular energy production.
Every cell in your body uses CoQ10. Your heart uses more of it than almost any other organ.
And statins slash your CoQ10 levels.
A meta-analysis published in the European Journal of Pharmacology in 2015 reviewed twenty-six clinical trials and confirmed it: statin therapy significantly reduces circulating CoQ10 levels.
The researchers noted that this depletion is dose-dependent — the higher the statin dose, the greater the CoQ10 loss.
That’s your cellular energy disappearing. And your doctor calls the resulting fatigue a mystery.
But it gets worse.
Cholesterol is the raw material your body uses to make steroid hormones. Testosterone. DHEA. Pregnenolone. Cortisol. All of them are built from cholesterol.
When you artificially suppress cholesterol production, you are suppressing the supply chain for every hormone that makes you feel like a man.
A study published in the Journal of Sexual Medicine in 2010 found that men on statins had significantly lower levels of bioavailable testosterone compared to matched controls.
Another study in Reproductive Biology and Endocrinology found statin use was associated with reduced testosterone and increased risk of hypogonadism symptoms.
Men taking statins are more likely to get type two diabetes. This is partly a result of the statins themselves and also a result of their lowering testosterone. Higher testosterone actually lowers a man’s chance of getting type two diabetes dramatically. Statins interfere with higher testosterone.
And then the pain: the muscle pain is real too.
It’s called statin-induced myopathy, and it affects anywhere from 7% to 29% of users depending on the study. A 2019 review in the Journal of Cachexia, Sarcopenia and Muscle found that statins accelerate muscle degradation through multiple mechanisms — mitochondrial dysfunction, increased muscle protein breakdown, and impaired muscle regeneration.
I recall a neighbor who was using a walker even though he was relatively young, around seventy. He said that his muscles had just fallen apart as soon as he was on statins and he stopped the statins several years ago, but the muscle never came.
And also...
Three favors before I continue.
Hit the ❤️. Substack’s algorithm will know that you like it, and show it to more people. Thank you for the like!
Hit the 🔄 restack. Your friends need to see this stuff about the pills they are taking.
Hit 📤 share. Somebody, one of your friends or family, is confronting serious health issues. My work has helped countless thousands go down the medical rat hole. You are doing them a favor!
And: Please leave a comment below. I read every one and I reply. I have 80,000 men I’ve helped and I’ve learned far more from them, than they have learned from me.
Okay…
When doctors hate statins
There’s also an excellent study where a few doctors were given statins. These are doctors that were prescribing statins routinely but never taken them themselves. When they were taking statins, they decided real quick that statins were a really bad idea. They had a ton of side effects and they realized that they had been making a mistake prescribing these to their patients.
So let me get this straight. A drug that depletes your cellular energy, lowers your testosterone, increases chances of getting type 2 diabetes, and breaks down your muscles. And it’s prescribed to over 40 million Americans.
Because a number on a lab test went up. Even though it’s healthy to have higher cholesterol, the real danger is lower cholesterol.
Sigh.
2. SSRIs — The Antidepressant That Kills Your Drive
Prozac. Zoloft. Lexapro. Paxil. Celexa.
Over 37 million Americans take an SSRI antidepressant. They are prescribed for depression, anxiety, OCD, panic disorder. Even premature ejaculation.
And increasingly, for things like mild situational sadness and stress that probably don’t require medication at all.
Here is what the research says about what these drugs do to men.
A landmark review published in Current Psychiatry analyzed the sexual side effects of SSRIs and found that between 25% and 73% of users experience sexual dysfunction. That includes reduced libido, difficulty achieving erection, difficulty reaching orgasm, and reduced genital sensation.
Between 25 and 73 percent. That is not a rare side effect. That is a defining feature of the drug class.
And here’s the part that should make your blood run cold.
A study published in the Journal of Clinical Psychiatry in 2006 documented what researchers call Post-SSRI Sexual Dysfunction — PSSD. These are sexual side effects that persist after the drug is discontinued. Months after. Years after. In some cases, indefinitely.
The researchers found that a subset of men who took SSRIs and then stopped experienced lasting changes in genital sensation, arousal, and orgasm function. Their serotonin receptors had been altered at a level that didn’t simply bounce back when the drug was removed.
Let me say that plainly.
There are men who took an antidepressant for six months and have not had normal sexual function in years.
And their doctors never warned them this was possible.
A 2018 study in the International Journal of Risk & Safety in Medicine provided further evidence, and the European Medicines Agency formally recognized PSSD as a potential long-term effect the same year.
But beyond sexual function, SSRIs create a broader problem. They blunt emotional range. The clinical term is “emotional blunting.”
A study in the Journal of Affective Disorders in 2017 found that nearly half of SSRI users reported feeling emotionally numb — reduced ability to feel pleasure, reduced ability to cry, reduced motivation, reduced creativity.
You came in because you were sad. The drug took away the sadness. But it also took away the joy. The drive. The fire. The thing that makes a man get up and fight for something.
That is not healing. That is chemical castration of the spirit.
In the search for headache relief, I took SSRIs (fluvoxamine and fluoxetine) in small amounts, practically microdoses, and I just could not believe how people could take these.
They caused me a great deal of gastrointestinal upset, which is a very common side effect.
And they completely interfered with my erections and sex drive. Awful stuff.
3. Proton Pump Inhibitors — The Acid Reflux Drug That Robs Your Body
Omeprazole. Pantoprazole. Esomeprazole. Brand names: Prilosec, Protonix, Nexium.
These are proton pump inhibitors — PPIs.
They are among the most prescribed drugs on earth. Over 15 million Americans have active PPI prescriptions, and millions more take them over the counter.
They were designed for short-term use — four to eight weeks for ulcers or severe reflux.
Of course, nobody has ever taken them for just a few weeks. People tend to take them for a few weeks and stay on them for years, many years.
And the consequences are stacking up.
PPIs work by shutting down the proton pumps in your stomach lining that produce hydrochloric acid. Less acid, less reflux. Simple. But stomach acid is not a design flaw. It exists for critical reasons.
The first problem with reduced stomach acid is that you increase the growth of harmful bacteria in your small intestine where they do not belong.
This causes a illness that mainstream doctors just ignore. It’s called SIBO, small intestinal bacterial overgrowth. Symptoms can include burping, indigestion, heartburn, the reasons you might have started the PPI in the first place.
Once you get SIBO, it’s hard to fix because these bacteria really like sticking around and it can lead to more of them in your actual stomach, including Helicobacter pylori, which is now known to be the cause of stomach ulcers. Another reason people take PPIs is because they have stomach ulcers, so it doesn’t make much sense, does it?
And actually most people I’ve worked with benefit from taking extra stomach acid, not inhibiting the stomach acid that they normally produce.
Low stomach acid is the most frequent cause of acid reflux.
And very, very easily fixed by taking hydrochloric acid in the form of betaine hydrochloride with protein meals.
You need stomach acid to absorb minerals also.
Magnesium. Calcium. Iron. Zinc. Without adequate acid, these minerals pass through your gut unabsorbed.This can increase the chances of getting osteoporosis, osteopenia, and also a magnesium deficiency.
A 2011 study published in JAMA Internal Medicine found that long-term PPI use was associated with a 25% increased risk of magnesium deficiency.
The FDA issued a formal safety warning that same year about hypomagnesemia in PPI users.
Why does that matter? Because magnesium is involved in over 300 enzymatic reactions in your body. It is essential for muscle function, nerve function, blood pressure regulation, blood sugar control, and — critically — testosterone production. Low magnesium is directly correlated with low testosterone.
A study in Biological Trace Element Research found that magnesium supplementation increased both free and total testosterone levels in men, and that the effect was even stronger in men who exercised.
So the PPI robs your magnesium. And the magnesium deficiency lowers your testosterone. And your doctor never connects the two.
It doesn’t stop there.
PPIs dramatically reduce B12 absorption.
A 2013 study in JAMA found that patients on PPIs for two or more years had a 65% increased risk of vitamin B12 deficiency. B12 deficiency causes fatigue, brain fog, memory problems, nerve damage, and depression. Symptoms that often get treated with — you guessed it — more prescriptions.
I have shown very easy ways to get rid of even severe acid reflux without taking these pills. I’ve done it myself and I’ve helped many people do it.
I’m not saying you should just stop taking the pills, but if you have our All Access Pass, you gain access and you will discover the exact method of using simple over-the-counter supplements to eliminate acid reflux and not need a PPI drug at all.
Click to get an All Access Pass trial.
And the kidney data is alarming.
A 2016 study in JAMA Internal Medicine followed over 10,000 patients and found that PPI use was associated with a 20-50% increased risk of chronic kidney disease.
A subsequent study found increased risk of acute kidney injury and end-stage renal disease.
All from a pill that most of these men could stop taking if they used some simple over the counter supplements.
4. Beta-Blockers — The Blood Pressure Drug That Kills Performance
Metoprolol. Atenolol. Propranolol. Carvedilol.
So often I work with men who complain about their erections. We discuss medications and I find out that they’re taking a beta blocker, and then I point out beta blockers can cause ED just by themselves.
There are many ways of fixing blood pressure without pills, but if you’re going to take pills, you may want to discuss a different one with your doctor because beta blockers all kill erections.
Despite this, beta-blockers are prescribed to over 30 million Americans for high blood pressure, heart rhythm issues, and sometimes anxiety.
They work by blocking the effects of adrenaline on your heart, slowing your heart rate and lowering blood pressure.
The side effect profile reads like a list of everything a man does not want.
A meta-analysis published in the Journal of the American College of Cardiology in 2002 reviewed fifteen clinical trials and found that beta-blocker therapy was associated with a significantly increased risk of erectile dysfunction compared to placebo.
The risk was highest with older-generation beta-blockers like atenolol, but present across the class.
The mechanism is straightforward. Erections require blood flow. Beta-blockers reduce cardiac output and blunt the sympathetic nervous system response that drives blood into the erectile tissue. They also lower norepinephrine, which plays a direct role in sexual arousal.
A study in the British Medical Journal found that men who were told about the erectile dysfunction risk of beta-blockers were significantly more likely to experience it. But here’s the key insight — men who were not told also experienced it at rates far higher than placebo. The nocebo effect made it worse, but the pharmacological effect was real.
Beyond sexual function, beta-blockers cause fatigue. Profound, leaden fatigue.
Because they block your body’s ability to respond to adrenaline, they reduce exercise capacity by 15-25% in studies.
They make it harder to work out.
Harder to push yourself.
Harder to build the muscle and lose the fat that would actually fix your blood pressure naturally.
They also contribute to weight gain.
A study in Hypertension found that patients on beta-blockers gained an average of 2.6 pounds more than patients on other antihypertensive classes over the study period.
And weight gain, as we covered in my last article, is one of the primary drivers of low testosterone.
So the drug prescribed for your blood pressure makes you fatter, more tired, and unable to perform in the bedroom — three things that make your cardiovascular health worse in the long run.
That is not a solution. That is a treadmill.
Not to mention, many other side effects.
By the way, blood pressure often rises as we get older, and it’s not necessarily a bad thing.
As men get into their seventies, eighties, higher blood pressure is protective and actually correlates with longevity.
Women in their seventies were found to live longer when they had hypertension. Men who are 75 or older lived longer with hypertension, especially higher systolic pressure, in one of several studies.
5. Finasteride — The Hair Loss and Prostate Drug With a Devastating Secret
Propecia. Proscar. Generic finasteride.
This is the one that makes me the angriest.
Finasteride is prescribed to millions of men for hair loss and enlarged prostate. It works by blocking the enzyme 5-alpha reductase, which converts testosterone into dihydrotestosterone — DHT.
DHT is the most potent androgen in a man’s body. It is supposedly responsible for male-pattern body hair, deepening of the voice during puberty, prostate growth — and yes, it plays a role in hair loss at the scalp.
Maybe. I doubt it does, but that’s what “they” say.
So the logic was simple: block DHT, save the hair.
But DHT is not a waste product. It is not a mistake your body makes. DHT drives libido. It supports sexual function. It affects mood, cognitive clarity, and neurological health. It is what makes testosterone actually work in many tissues.
And finasteride crushes it.
A study published in the Journal of Sexual Medicine in 2011 surveyed 71 men who had taken finasteride for male-pattern hair loss.
Of those men, 92% reported new-onset sexual dysfunction during use — including low libido, erectile dysfunction, and problems with orgasm.
But here is the devastating part.
In that same study, 89% of the men who reported sexual dysfunction said the problems persisted after stopping the drug.
The median duration of finasteride use was 28 months. The median duration of persistent side effects at the time of the study was 40 months — and counting.
They call this Post-Finasteride Syndrome — PFS. And while the pharmaceutical industry spent years dismissing it, the evidence kept piling up.
A 2012 study in The Journal of Clinical Endocrinology & Metabolism found that men with PFS had altered levels of neuroactive steroids in their cerebrospinal fluid.
The drug had changed their brain chemistry — specifically, the neurosteroids that regulate mood, anxiety, and sexual function. These changes persisted long after the drug was cleared from their system.
A 2015 study in PeerJ found that former finasteride users had persistent changes in gut bacteria and androgen metabolism markers.
A study in The American Journal of Men’s Health documented cases of depression, anxiety, cognitive impairment, and suicidal ideation in post-finasteride patients.
Let me be clear about what happened here.
Young men — many of them in their twenties and thirties — went to a doctor because they were losing their hair. A cosmetic concern. And they were given a drug that, in a significant subset, destroyed their sexual function, altered their brain chemistry, and left them with symptoms that have lasted years.
The Post-Finasteride Syndrome Foundation has collected thousands of reports. In 2022, Reuters conducted an investigation that found the FDA had received tens of thousands of adverse event reports for finasteride — including reports of persistent sexual dysfunction and suicidality.
And it is still prescribed every day. Without adequate warnings. Without informed consent about the risk of permanent side effects.
There are other drugs such as dutasteride and tamsulosin that have similar risks, especially given for prostate issues. Personally I would never take them.
I have helped thousands of men fix prostate issues and hair loss issues without drugs like this.
The Pattern You Need to See
Step back and look at what I just showed you.
Five of the most commonly prescribed drugs in America. Taken by tens of millions of men. And every single one of them has documented effects on testosterone, sexual function, energy, or the nutrients your body needs to produce hormones.
Statins lower your CoQ10 and your testosterone, they raise chances of getting debilitating muscle disease and diabetes.
SSRIs kill your drive and may permanently alter your sexual function.
PPIs rob you of the minerals you need to make hormones.
Beta-blockers make you fat and impotent.
Finasteride can chemically castrate you for years.
And in many cases, these drugs are prescribed for conditions that could be addressed — or significantly improved — through lifestyle changes. Weight loss. Diet. Exercise. Sleep. Stress management.
But lifestyle changes don’t generate $400 billion a year in pharmaceutical revenue.
I’m not telling you to flush your prescriptions down the toilet. Some of these drugs save lives in specific circumstances. Beta-blockers after a heart attack. SSRIs during a genuine psychiatric crisis. Statins for men with familial hypercholesterolemia and documented cardiovascular disease.
But the casual, long-term, population-wide prescribing of these drugs to men whose underlying problems are metabolic?
That is not medicine.
That is a factory medicine system that is broken.
And the man on the factory assembly line -- he is losing things he doesn’t even know he’s losing — until one day he wakes up exhausted, overweight, unable to perform, unable to feel, and his doctor tells him it’s normal at his age.
It’s not his age.
It might be his medicine cabinet.
What To Do
If you are on any of these medications, the first step is not to stop taking them. The first step is to ask why you’re on them.
Talk to your doctor — or find a better one — and ask the question most patients never ask: “What would it take for me to not need this drug?”
For statins: Is your cardiovascular risk actually high enough to justify the side effects? I can’t really imagine a justification for anyone taking them honestly.
For SSRIs: Is your depression situational or clinical?
Have you tried exercise — which meta-analyses show is as effective as SSRIs for mild to moderate depression?
Are you aware of the sexual side effect risk, including the risk of persistence?
For PPIs: Are you still taking this years after it was prescribed for a two-month course?
Have you tried eliminating trigger foods, eating earlier, elevating the head of your bed? Has anyone checked your magnesium and B12?
For beta-blockers: Could your blood pressure be managed with weight loss, exercise, and dietary changes? Are you aware of the sexual and metabolic side effects?
For finasteride: Is keeping your hair worth the documented risk to your sexual function, mood, and neurological health? Has anyone given you true informed consent about Post-Finasteride Syndrome?
These are not radical questions. These are the questions your doctor should be asking before reaching for the prescription pad.
In most cases, we need to improve sleep, move around a bit, eat real food, drink clean water, and try to avoid stress in our life.
Fix the foundation first. And question every pill that’s sitting between you and the man you’re supposed to be.
Citations
1. Banach M, et al. “Effects of coenzyme Q10 on statin-induced myopathy: a meta-analysis of randomized controlled trials.” Mayo Clinic Proceedings, 2015. https://pubmed.ncbi.nlm.nih.gov/25440725/
2. Corona G, et al. “The Effect of Statin Therapy on Testosterone Levels in Subjects Consulting for Erectile Dysfunction.” Journal of Sexual Medicine, 2010.
3. Needham M, Mastaglia FL. “Statin myotoxicity: a review of genetic susceptibility factors.” Neuromuscular Disorders, 2014. https://pubmed.ncbi.nlm.nih.gov/24290403/
4. Serretti A, Chiesa A. “Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis.” Journal of Clinical Psychopharmacology, 2009.
5. Csoka AB, Shipko S. “Persistent sexual side effects after SSRI discontinuation.” Psychotherapy and Psychosomatics, 2006.
6. Healy D, et al. “Enduring sexual dysfunction after treatment with antidepressants, 5α-reductase inhibitors and isotretinoin: 300 cases.” International Journal of Risk & Safety in Medicine, 2018.
7. Goodwin GM, et al. “Emotional blunting with antidepressant treatments: A survey among depressed patients.” Journal of Affective Disorders, 2017.
8. Lam JR, et al. “Proton Pump Inhibitor and Histamine 2 Receptor Antagonist Use and Vitamin B-12 Deficiency.” JAMA, 2013.
9. Lazarus B, et al. “Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease.” JAMA Internal Medicine, 2016.
10. Cinar V, et al. “Effects of Magnesium Supplementation on Testosterone Levels of Athletes and Sedentary Subjects at Rest and after Exhaustion.” Biological Trace Element Research, 2011.
11. Ko DT, et al. “Beta-Blocker Therapy and Symptoms of Depression, Fatigue, and Sexual Dysfunction.” Journal of the American Medical Association, 2002.
12. Irwig MS, Kolukula S. “Persistent Sexual Side Effects of Finasteride for Male Pattern Hair Loss.” Journal of Sexual Medicine, 2011.
13. Melcangi RC, et al. “Neuroactive Steroid Levels and Psychiatric and Andrological Features in Post-Finasteride Patients.” Journal of Sexual Medicine, 2013. https://pubmed.ncbi.nlm.nih.gov/23890183/
14. Ganzer CA, et al. “Persistent Sexual, Emotional, and Cognitive Impairment Post-Finasteride.” American Journal of Men’s Health, 2015.
15. Yi SW, Yi JJ, Ohrr H. “Total cholesterol and all-cause mortality by sex and age: a prospective cohort study among 12.8 million adults.” Scientific Reports, 2019. https://pubmed.ncbi.nlm.nih.gov/30733566/
16. Langer RD, Ganiats TG, Barrett-Connor E. “Factors Associated with Paradoxical Survival at Higher Blood Pressures in the Very Old.” American Journal of Epidemiology, 1991. https://academic.oup.com/aje/article-abstract/134/1/29/90292
17. Langer RD, Ganiats TG, Barrett-Connor E. “Paradoxical survival of elderly men with high blood pressure.” BMJ, 1989. https://pmc.ncbi.nlm.nih.gov/articles/PMC1836610/
Yikes.
Great post 👍.